
Your Psychotherapy Notes Don't Write Themselves. Until Now.
Your Psychotherapy Notes Don't Write Themselves. Until Now.
Why clinical psychologists in the Philippines carry one of the heaviest documentation burdens in healthcare — and what's finally changing that

There's a particular kind of exhaustion that clinical psychologists and counsellors rarely talk about in public. It's not the exhaustion of sitting with someone in crisis, or holding space for trauma that would break most people. That part — the actual therapeutic work — is what they trained for.
The exhaustion comes after. When the session ends, the client leaves, and the clinician sits down to reconstruct everything that just happened from memory. The presenting issue. The emotional state. The interventions tried. The client's response. The plan for next time. All of it typed out in structured clinical language, often for multiple clients in a row, at the end of a day that was already full.
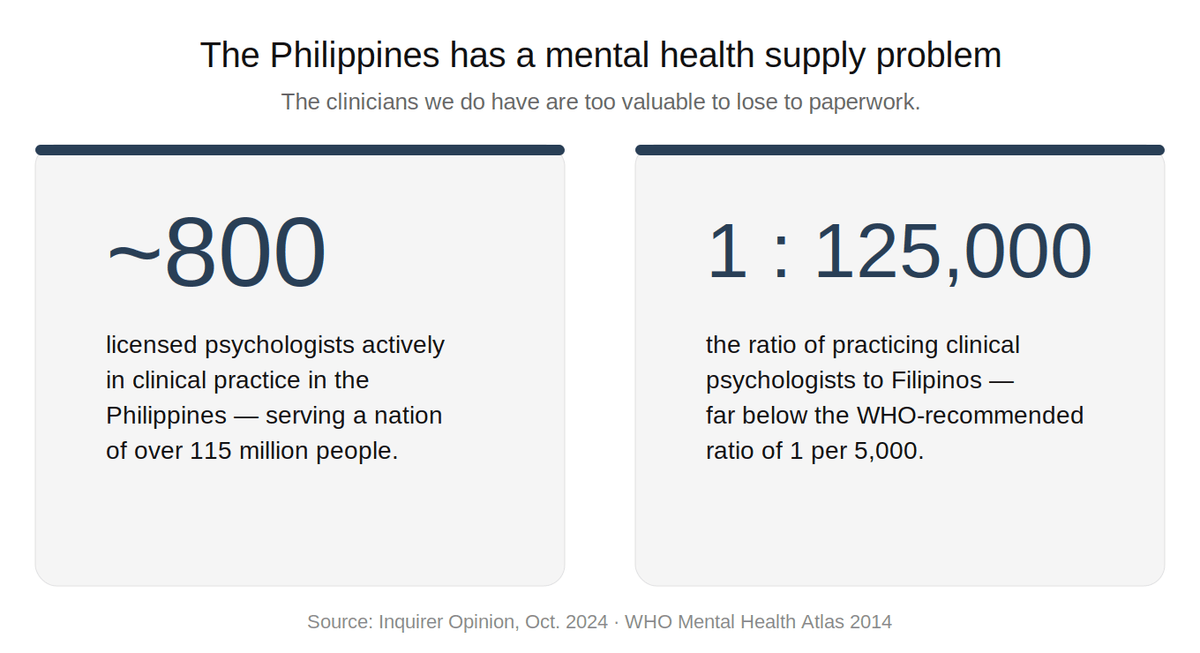
This is the documentation burden in mental health. And in the Philippines, it lands on a profession that is already stretched thin.
The Philippine Context
The Philippines has fewer than 1,000 licensed clinical psychologists serving a population of over 115 million. The passage of the Mental Health Act (Republic Act 11036) in 2018 was a watershed moment — it formally recognized mental health as a public health priority and expanded the mandate for psychological services across schools, workplaces, and communities. But the law created demand faster than the system could create supply.
The result: the clinical psychologists and registered guidance counsellors who do practice are often running full caseloads, sometimes across multiple settings — private practice, hospitals, academe, corporate wellness. Each session generates documentation requirements. Each client file needs to be maintained. And unlike general medicine, where a consultation note might take five minutes to complete, a therapy session note is a different kind of task entirely.
Why Mental Health Notes Are Different
In clinical psychology, what matters most is often what wasn't said out loud. The shift in affect when a particular topic came up. The way a client deflected. The moment a breakthrough started forming, then retreated. The subtle progress that doesn't announce itself but needs to be documented to be tracked over time.
Translating that into a structured note — whether DAP format, BIRP, GIRP, PIRP, or a narrative progress note — requires active reconstruction. The clinician has to hold the arc of a 50-minute conversation in their head, find the clinical through-line, and render it in language that is both therapeutically accurate and professionally defensible.
Do that eight times a day and it stops being administrative overhead. It becomes a cognitive tax on the very capacities — attunement, presence, emotional range — that the work demands.
The Presence Problem
Here's what the documentation burden actually costs, beyond time.
A therapist who knows they have five session notes to write after their last client is already carrying that weight in the room. Not consciously, not always — but the knowledge of what's waiting on the other side of a session creates a low-grade cognitive pull that competes with full therapeutic presence.
Presence is not a soft concept in clinical psychology. It's a clinical variable. The quality of attunement between therapist and client has been consistently shown to be one of the strongest predictors of therapeutic outcome — stronger, in many studies, than the specific modality used. A therapist who is partially elsewhere, even by a small degree, is a less effective therapist.
The documentation burden doesn't just cost time. It costs presence. And in a field where presence is the mechanism, that's not a trivial loss.
What an AI Scribe Actually Does in a Therapy Context
The idea of AI in a therapy room can feel instinctively wrong. Therapy is intimate. It depends on confidentiality, trust, and the sense that what happens in the session stays there. Any technology that enters that space needs to earn its presence.
Done correctly, an ambient AI scribe doesn't intrude on that. It listens in the background with explicit client consent, captures the session, and does the structural work of documentation so the clinician doesn't have to reconstruct it from scratch afterward. The therapeutic conversation remains what it always was — between two people, in a room, without an audience.
What changes is what happens after.
Instead of spending 20 to 30 minutes per session converting memory into structured notes, the clinician opens a draft. A DAP note organized around the session's data, assessment, and plan. A progress note that tracks movement against treatment goals over time. A session summary that captures presenting concerns, interventions, and client response. All of it generated from the session itself — not invented, not hallucinated, but structured from what was actually said.
The clinician reviews, edits, confirms. The clinical judgment stays entirely theirs. The AI handles the scaffolding.
The Compounding Effect
The benefit isn't just per session. It compounds.
A therapist who isn't carrying documentation debt into each new session has more cognitive and emotional bandwidth available. Over weeks and months, that difference is measurable — in the quality of sessions, in the sustainability of a full caseload, in the simple fact of not ending every working day depleted by paperwork rather than the work itself.
Mental health clinician burnout is a serious and growing problem in the Philippines and across Southeast Asia. The contributing factors are well-documented: high emotional load, inadequate systemic support, and administrative burden that consumes time meant for clinical work or recovery. AI-assisted documentation doesn't solve all of those. But it addresses one of the most tractable ones directly.
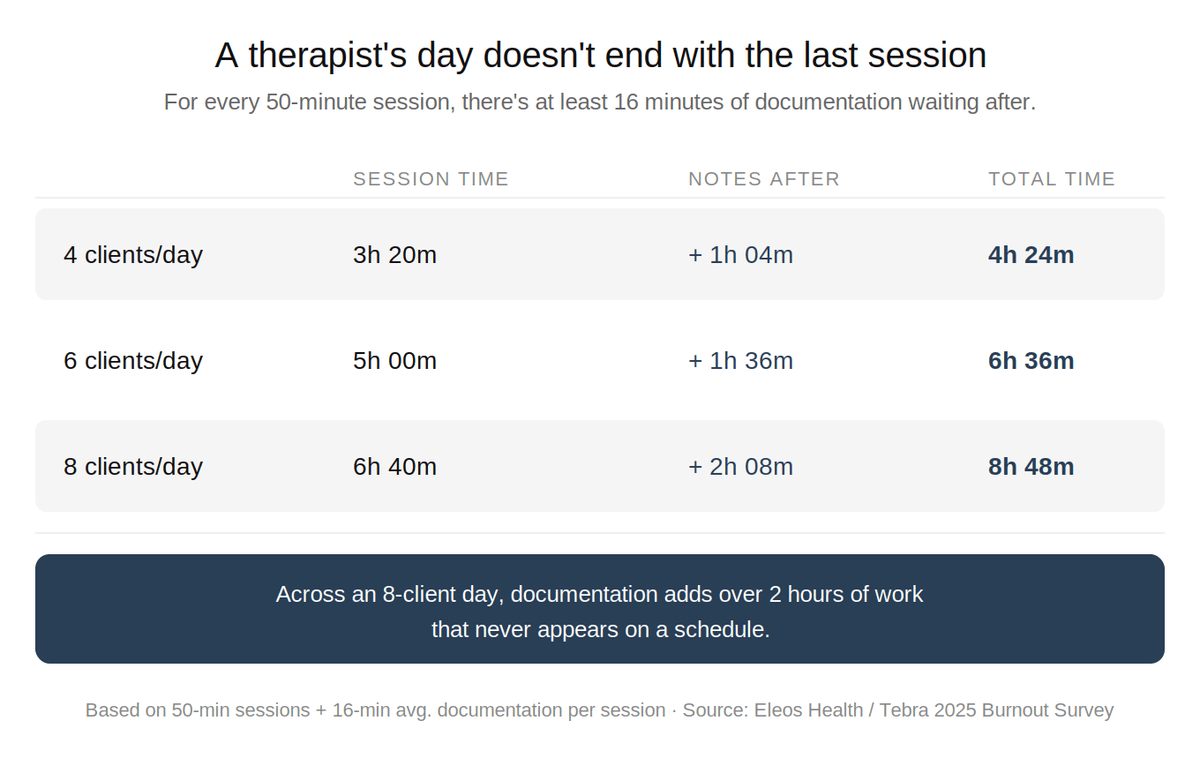
Eleos Health, which has analyzed documentation patterns across thousands of mental health clinicians, found that therapists spend approximately 35% of their total working hours on documentation — roughly 16 minutes per client encounter at the encounter level, before accounting for treatment plan updates, coordination letters, and intake assessments. In a 30-client week, that's more than 8 hours of documentation alone. Inquirer Opinion
Tebra's 2025 Burnout Survey found that mental health clinicians report the highest rates of mental fatigue of any medical specialty — 77% meet criteria for significant mental exhaustion, with documentation and charting cited as the leading burnout driver by 23% of respondents.
For private practice psychologists and counsellors in particular — who carry both the clinical load and the operational weight of running their own practice — removing the documentation overhead can be the difference between a sustainable practice and one that quietly grinds the clinician down.
A Note on Format
Clinical psychology documentation isn't one-size-fits-all. Different settings, supervisors, and clinical frameworks call for different note structures. DAP is common in counselling and private practice contexts. BIRP and GIRP are used in behavioral health and structured therapeutic programs. PIRP is standard in some psychiatric and rehabilitation settings.
A well-designed AI scribe doesn't impose a single format — it adapts to the clinician's workflow and the documentation standard their practice requires. The goal isn't to make every session note look the same. It's to make sure the clinician isn't the one doing the structural heavy lifting after every single session.
The Larger Argument
There's a version of this conversation that focuses narrowly on efficiency — minutes saved per session, notes completed per day. That framing isn't wrong, but it misses the more important point.
The best therapeutic work happens when the clinician is fully present. Fully present requires not being depleted. Not being depleted requires that the work after the session doesn't cost as much as the session itself.
For Filipino clinical psychologists already navigating a system that asks much and gives back little in terms of infrastructure and support, that equation matters more than anywhere. AI-assisted documentation in clinical psychology isn't about making therapy faster. It's about making the conditions for good therapy more sustainable — for the clinician, and by extension, for every client they see.
The session is where the healing happens. The note is just the record. It shouldn't be the hardest part of the day.
AI-powered language aware clinical documentation built for south-east asian clinicians
BetterClinic listens to your consultations, generates structured SOAP notes and differential diagnoses in real time, and handles PhilHealth compliance — so you spend less time on paperwork and more time with patients.Surye?